

Story
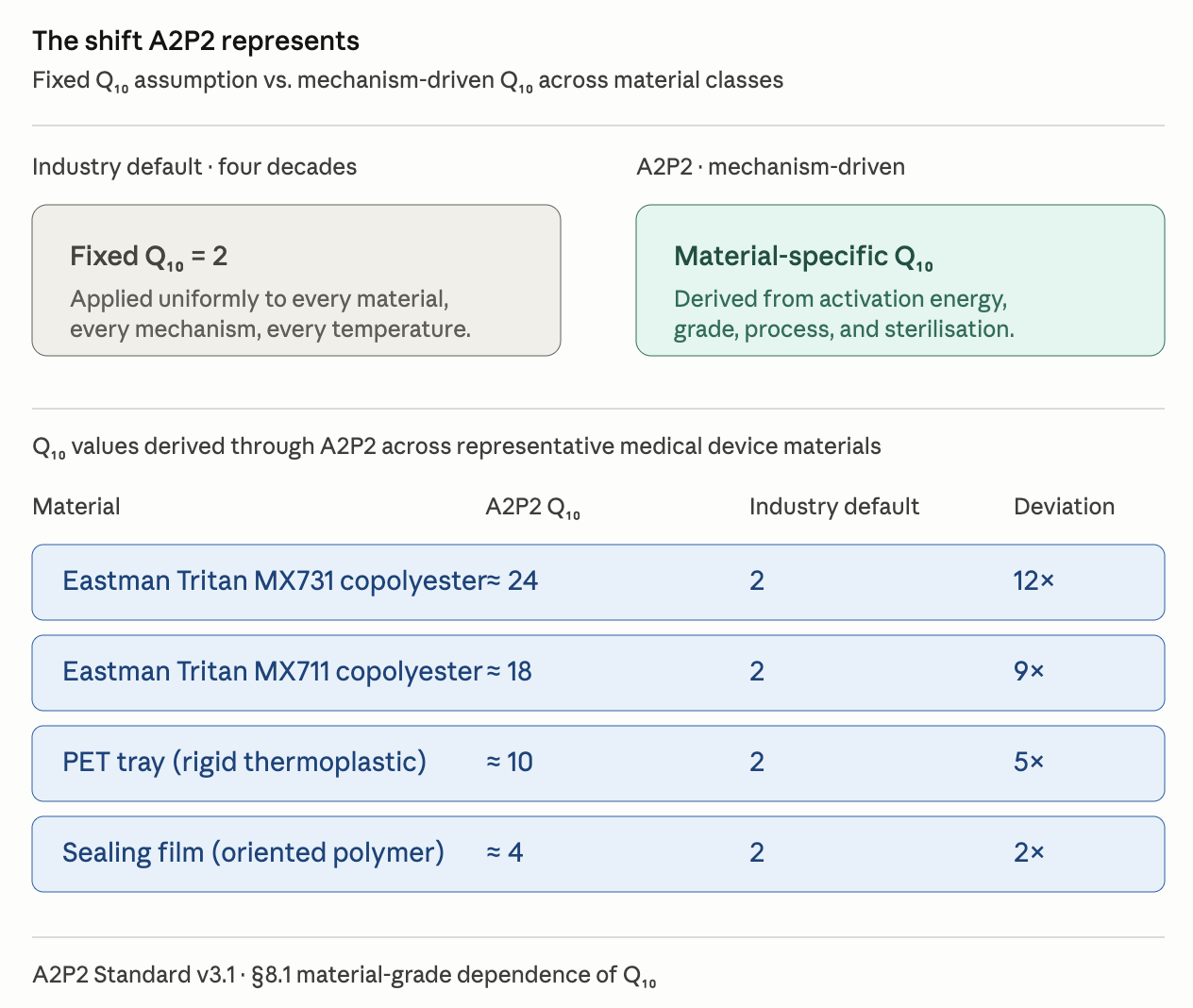
The Q₁₀ = 2 assumption — that material ageing rates double for every 10°C rise in temperature has underpinned accelerated stability testing in the medical device industry for four decades. It was adopted because it was conservative, computationally trivial, and applicable across material classes that the field had no better way to distinguish. For most of that period, it was the most rigorous tool available.
It is no longer.
The materials-science evidence accumulated steadily through the 2000s and 2010s. Activation energies for different polymer grades, processed differently and sterilised differently, were shown to vary by an order of magnitude. The fixed-Q₁₀ assumption was applying a single coefficient to systems whose underlying physics demanded individual treatment. Over-aged components were producing non-representative failure modes. Submissions were being delayed by test designs that the physics could not justify. The standards bodies knew, but the work of replacing the assumption with a mechanism-driven framework — derived from first principles, validated against field data, structured for regulatory adoption — had not yet been done.
That is the work A2P2 represents.
The framework is the product of fifteen years of polymer ageing research, structured progressively into a methodology that any team with standard DMA, DSC, FTIR, and GPC capability can apply. Three patents were filed to protect the computational architecture. The framework was validated against independent literature (Mishra et al., 2015), against four internal case studies spanning sterile barrier systems and implantable polyurethanes, and against eight years of continuous field service data from a polyamide composite separation membrane in pharmaceutical-grade water service. It was submitted to the FDA in March 2026 as Medical Device Development Tool submission, and the revised proposal is under active review. It is referenced in Section 6.4 of the ASTM F1980 revision, currently in ballot.
I am the Ambassador to ASTM F1980, the UK Expert to ISO/TC 194/WG 1 on medical device lifecycle, and a member of the BSI CH/194 committee on biological evaluation of medical devices. The standards process is slow by design: consensus protects the patients who depend on it.
But the cost of waiting is borne by the patients too, and the framework has reached the point where qualifying organisations can begin applying it in regulatory submissions today, ahead of the formal revision publication.
That is why A2P2 is licensed.
Dr Nazli Gulsine Ozdemir CEng FIMMM · London · 2026

Because the people who are crazy enough to think they can change the world, are the ones who do.
Steve Jobs